

Esophageal Laceration (“pre-Boerhaave’s Syndrome”) Treated with “Short-Stem” Hemoclips
By Hiral Patel, MD and Klaus Mönkemüller, MD, PhD, FASGE, FJGES
Virginia Tech Carilion School of Medicine, Virginia, USA
80-year-old patient with history of recent myocardial infarction, coronary stent placement and dual antiplatelet therapy presented with melena, hypotension and drop in hemoglobin from 14 gr/dl to 9 gr/dl. Emergent EGD showed a distal peptic stricture of the esophagus, which did not impede the passage of the scope (Fig. 1A and Fig. 1B). On retroflexion there was not Mallory-Weiss tear (Fig. 1C). Inspection of the distal esophagus revealed a 4 cm long laceration with adherent blood clots and visible vessel (Fig. 1D and Fig. 1E).
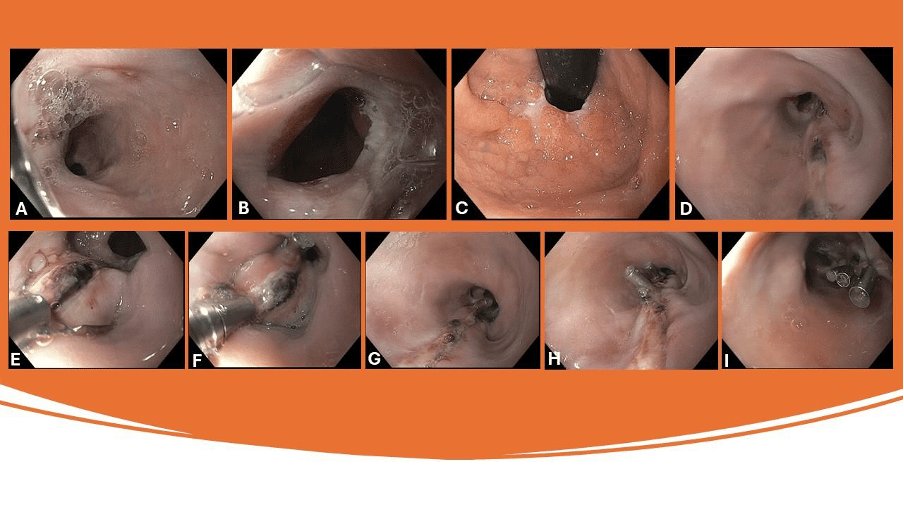
Image via EndoCollab.com
The laceration was clearly located 3 cm above the Z-line and GE junction. Occasionally, large esophageal erosions or ulcers in the setting of reflux esophagitis may appear similar to a laceration, but in GERD the erosion usually starts at the GE junction. Esophageal lacerations have a spectrum, from mucosal, submucosal, and muscle, to complete perforation or rupture (Boerhaave’s syndrome). Boerhaave’s syndrome is the extreme outcome of an esophageal laceration.
This patient had clear indication for endoscopic therapy: a) severe hemorrhage and b) lesion with high-risk stigmata. In this case we selected clips with short stems (or barrels) (yellow oval) to prevent luminal rubbing from the deployed clips (DuraClip). Figure 2 shows various commercially available clips and their stem lengths.
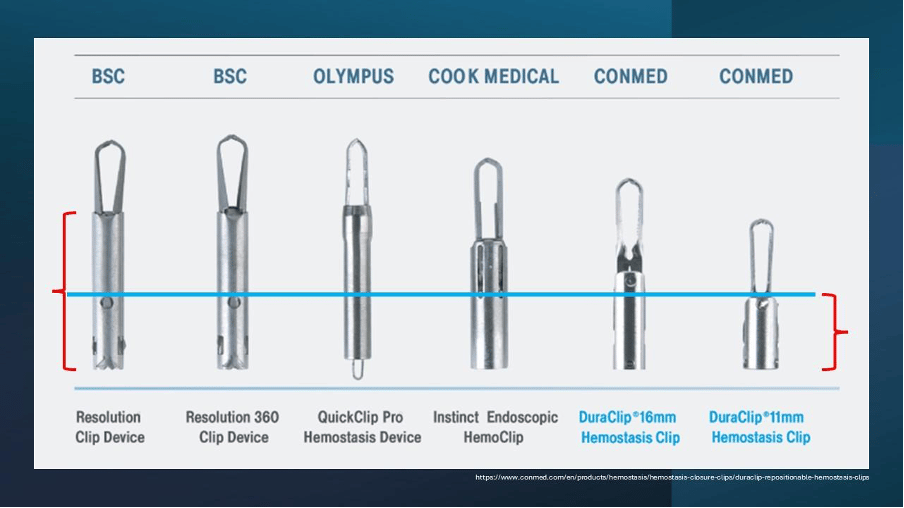
The DuraClip has some interesting and nice features. It is easily rotatable, even the scope is in retroflexion. It can open and close repeatedly, up to 50 times. This is a very convenient feature, as it allows the endoscopist to be 100% sure of the desired placement location (vessel, base of polyp, wound closure, etc). Indeed, in this case we had to open and close the clips several times because the borders of the laceration were hardened and we wanted to ensure a symmetrical and strong apposition of the tor edges. Additionally, this clip has a short stem (or barrel) which makes it ideal for esophageal work, because once it is deployed the stem will not rub the contralateral mucosa (Fig. 1H, Fig. 1I, Fig. 2). Lastly, the clip may also be rotated, which is ideal for approaching the borders of the defect.
References:
Xavier AT, Campos JF, Robinson L, Lima EJM, da Rocha LCM, Arantes VN. Endoscopic clipping for gastrointestinal bleeding: emergency and prophylactic indications. Ann Gastroenterol. 2020 Nov-Dec;33(6):563-570. doi: 10.20524/aog.2020.0526. Epub 2020 Jul 30. PMID: 33162733; PMCID: PMC7599350.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7599350/pdf/AnnGastroenterol-33-563.pdf
No COI by HP or KM with any of the companies/utensils or products mentioned in this article.
Take Your Endoscopy Practice to the Next Level with EndoCollab
Unlock a vast library of endoscopy resources, including:
1000+ endoscopy strategies
1100+ endoscopists from around the world
Constantly growing video course library
Comprehensive Endoscopy Atlas
Join the EndoCollab community today and start transforming your practice:
Monthly Plan: $14.99/month
Yearly Plan: $149.00/year (save 2 months)
Lifetime Access: $399.00 one-time payment (no recurring fees)