

Foreign Body Ingestion: When to Perform Endoscopy?
Welcome to this week’s journal review from EndoCollab. Today we distill a 12-year Israeli cohort that sharpens our decision-making around foreign-body ingestion. Key takeaway: any object lodged in the esophagus—or longer than 3.5 cm proximal to the duodenum—rarely passes on its own and warrants prompt endoscopic removal. Paid members unlock our full archive, videos, and an active chat thread where GI colleagues trade tips in real time. Ready for the deeper dive? Upgrade and join us.
Foreign body ingestion in adults is one of the most common emergencies confronted by the practicing endoscopist.
It is still not clear when a wait and watch strategy appropriate is.
In a large, retrospective study spanning 12-years Sbeit et al from Israel explored predictors for spontaneous passage of ingested foreign bodies by focusing on foreign body type, length, and location of impaction.
Overall, 365 patients with foreign body ingestion were included.
The rate of spontaneous passage was 53.7% in general, while the spontaneous passage rate was 47.9% in food impaction, 44.3% in sharp objects, 88.7% in blunt objects and only 22.2% in long blunt objects (> 6 cm).
On regression analysis, esophageal location was associated with a higher impaction rate and lower spontaneous passage vs. stomach and small and large intestine.
Performing Receiver operating characteristics (ROC) analysis found that the maximal length above which the foreign body will fail to pass spontaneously was 3.5 cm in the stomach and 3 cm in the small intestine.
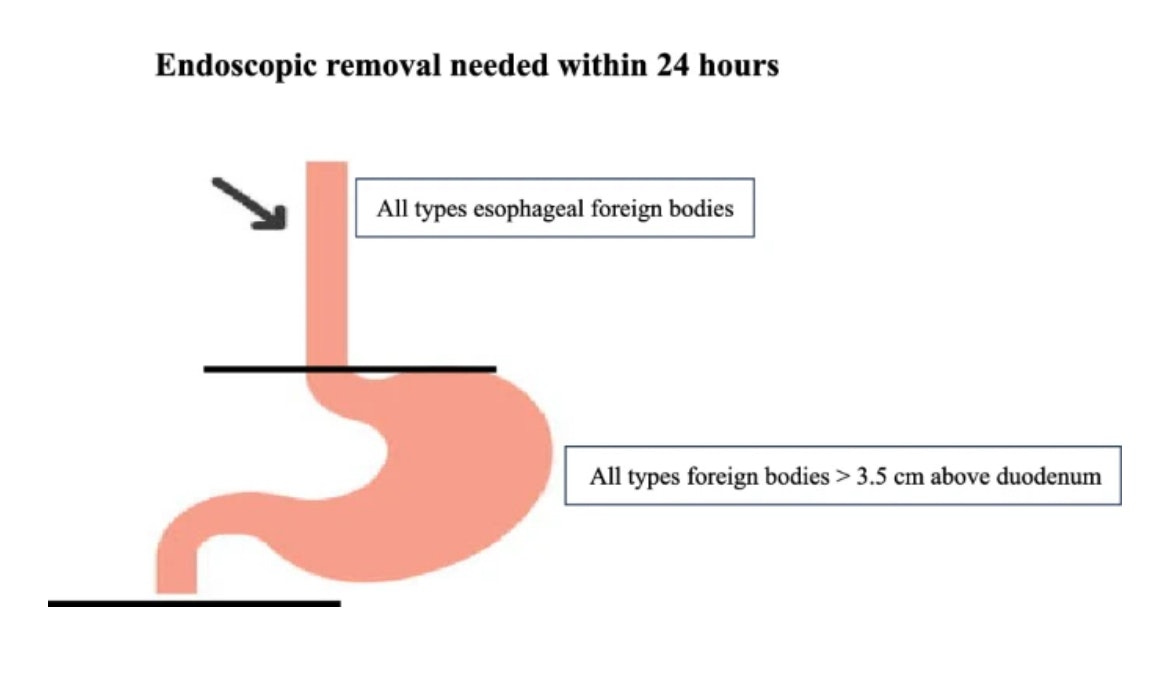
The authors concluded that endoscopic removal was needed for all esophageal foreign bodies, and all foreign bodies more than 3.5 cm above the duodenum. Spontaneous passage of ingested foreign body in a selected cohort of patients depends on foreign body type, location, and length.
Source: https://link.springer.com/article/10.1007/s00464-023-10657-y
Join the Members-Only Discussion
How do you balance “watch-and-wait” versus immediate retrieval for sharp, food-bolus, or battery ingestions? Do you use length cut-offs or rely more on location and patient factors? Share your protocol, toughest cases, or tool preferences so we can refine our collective playbook. See you in the comments!