

The 4-14-4 Rule to Obtain Esophageal Biopsies to Diagnose Eosinophilic Esophagitis
Journal Review
Welcome to this week’s journal review from EndoCollab. We’re spotlighting a deceptively simple protocol—the “4-14-4 rule” of eight esophageal biopsies—that boosted eosinophilic esophagitis detection 50-fold in Denmark with almost no extra workload. Free readers can skim the key take-aways below; paid members unlock our full archive, step-by-step video walk-throughs, and the chance to trade real-world tips with thousands of GI colleagues. If that sounds valuable, consider joining the EndoCollab community today.
In the North Denmark Region (580 272 inhabitants), only 0–4 cases of possible eosinophilic esophagitis (EoE) were identified annually in 1999–2010, suggesting underdiagnosis. This study aimed to increase the diagnosis of EoE by introducing a regional biopsy protocol for patients with dysphagia.
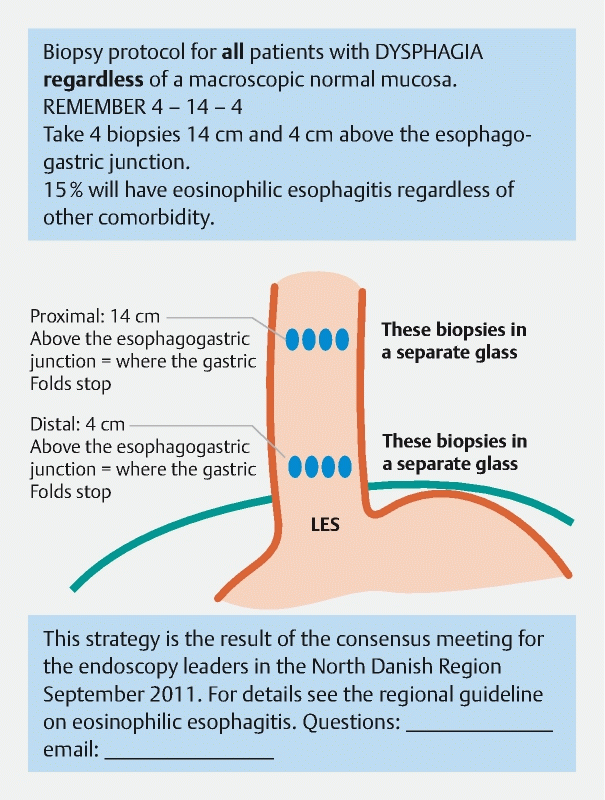
In 2011, leaders of regional endoscopy units attended a consensus meeting where a biopsy protocol was proposed to take eight biopsy samples in dysphagia patients (four biopsies from 4 cm and 14 cm above the esophagogastric junction–“4–14–4 rule”) regardless of the macroscopic appearance. A pictogram showing the 4–14–4 rule was sent to all endoscopy units.
The number of patients with esophageal eosinophilia detected per year increased 50-fold after the protocol was implemented in 2011 (median of 1 [interquartile range 0–3] vs. 52 [47–56]; P < 0.001), and the number of biopsy samples per patient doubled (median 4 [4–5] vs. 8 [6–9]; P < 0.04). Of 309 patients diagnosed with esophageal eosinophilia in 2007–2017, 24 % had erosive esophagitis or Barrett’s esophagus, and 74 % had EoE.
These patients can now receive treatment. The effort to establish the protocol and change the culture of endoscopists and pathologists was minimal (1).
1. Krarup et al. Endoscopy 2021 DOI: 10.1055/a-1206-0852
https://www.thieme-connect.com/products/ejournals/html/10.1055/a-1206-0852
Join the Members-Only Discussion
How many biopsies do you routinely take for unexplained dysphagia? Have you tried a systematic 4-14-4 approach, or found another strategy that works in your unit? Post your protocol, share stumbling blocks, or ask a question that could move the practice forward. Let’s build a practical playbook together—see you in the comments!