

The Setup: When Standard Cannulation Won’t Work
You’re staring at a bulging, floppy papilla dangling out of a periampullary diverticulum. The orifice points distally, blood is oozing from the base, and your standard sphincterotome just isn’t going to cooperate with this anatomy. What do you reach for — and more importantly, do you know the hidden cannulation trick built into that instrument that even many experienced endoscopists miss?
The case begins with a Type 3 (protruding) papilla — markedly bulging and physically hanging out of a diverticulum. Blood at the base suggested a stone had recently passed. Endoscopic ultrasound (EUS) confirmed additional stones in the bile duct.
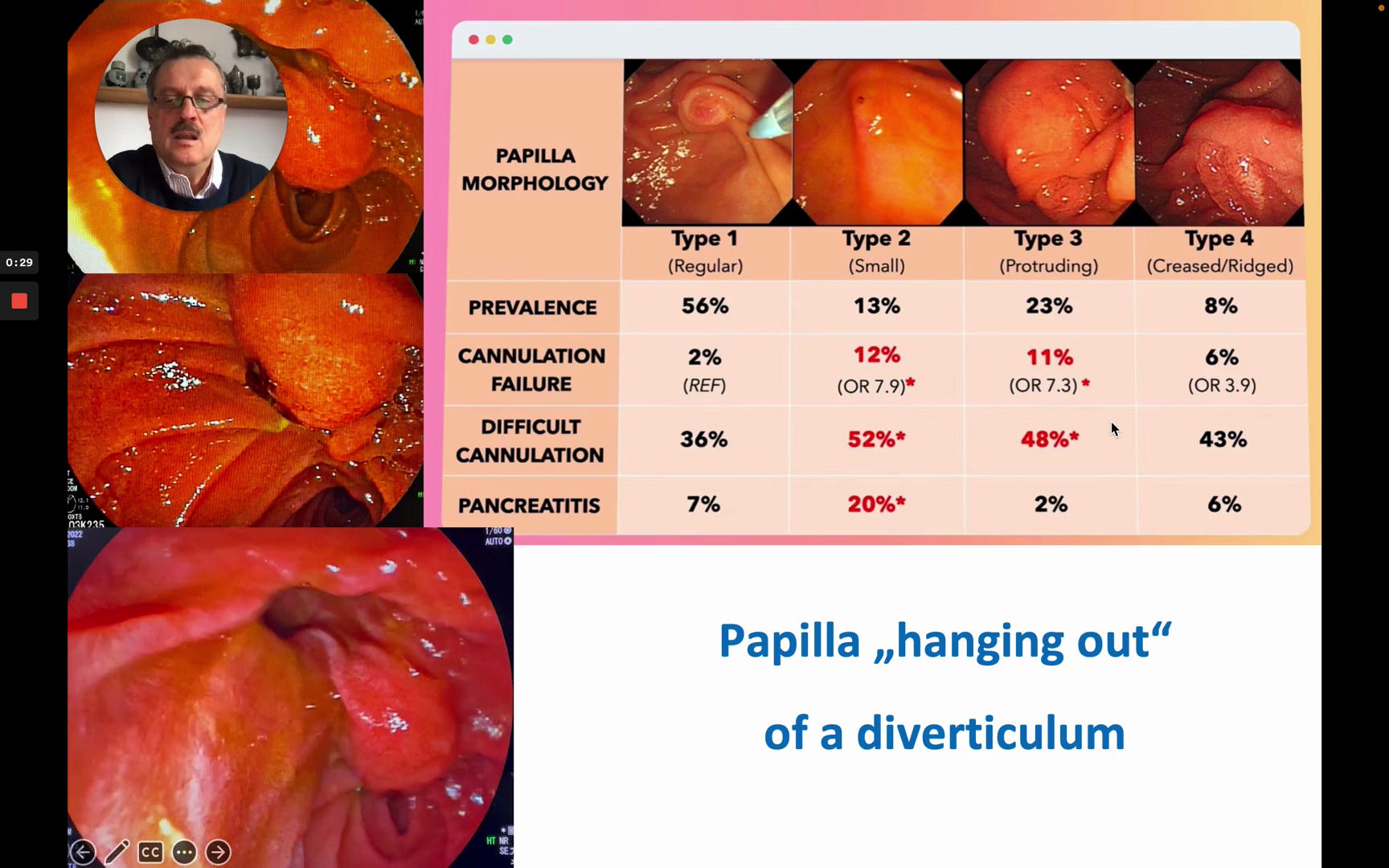
A papilla morphology classification table showing four types: Type 1 (Regular, 56% prevalence, 2% cannulation failure), Type 2 (Small, 13% prevalence, 12% cannulation failure with OR 7.9*), Type 3 (Protruding, 23% prevalence, 11% cannulation failure with OR 7.3*), and Type 4 (Creased/Ridged, 8% prevalence, 6% cannulation failure with OR 3.9). Difficult cannulation rates are 36%, 52%, 48%, and 43% respectively. Pancreatitis rates: 7%, 20%*, 2%, 6%. Below the table, an endoscopic image shows a papilla “hanging out” of a diverticulum.
Because of the floppy consistency, the hanging orientation, and the distally pointing orifice, starting with a standard sphincterotome was not a viable first approach. The decision was made to use the Huibregtse needle knife.
Why This Instrument: The Huibregtse Needle Knife
This knife is special because it is very useful both for cutting and for cannulation — a dual purpose that sets it apart from conventional needle knives.
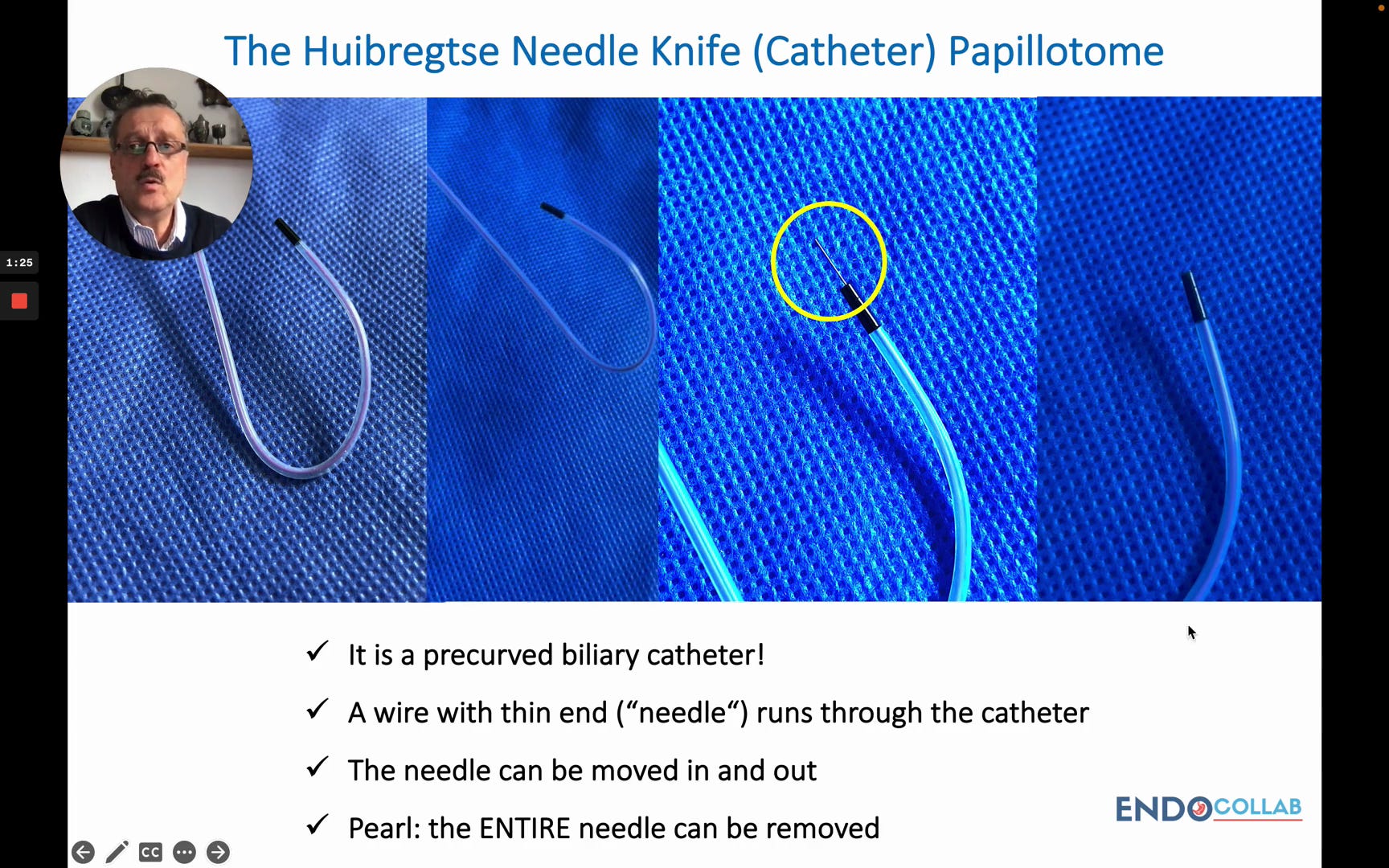
Close-up photographs of the Huibregtse Needle Knife on a blue sterile drape. Four progressive views show the full pre-curved biliary catheter, the catheter body, the tiny needle tip highlighted within a yellow circle, and a magnified distal view. Key features: “It is a precurved biliary catheter!” / “A wire with thin end (’needle’) runs through the catheter” / “The needle can be moved in and out” / “Pearl: the ENTIRE needle can be removed.”
As the speaker explains, inside the catheter runs a wire whose distal portion is a very small-diameter segment — the “needle.” Crucially, this entire needle-wire assembly can be completely removed after the cutting phase is finished, converting the device into a standard cannulation catheter.
To access the full step-by-step technique, the advanced “hanging papilla” approach, and a downloadable quick-reference guide based on this video, consider becoming a paid subscriber.
