

You’ve just deployed your Dormia basket. The stone is large, the duct is sclerosed, and now the basket won’t budge. The endoscope is locked in place. Your patient is on the table. Do you know what to do next?
Basket impaction is one of the most feared complications in ERCP (endoscopic retrograde cholangiopancreatography). But according to Dr. Mönkemüller, it is also largely preventable—and when it does occur, entirely salvageable—if you’ve prepared in advance. This presentation covers two critical skill sets: anticipating mechanical problems before they happen, and executing a systematic rescue when they do.
Anticipating Mechanical Problems Before You Begin
The foundation of safe biliary stone management is pre-procedural cholangiogram analysis.
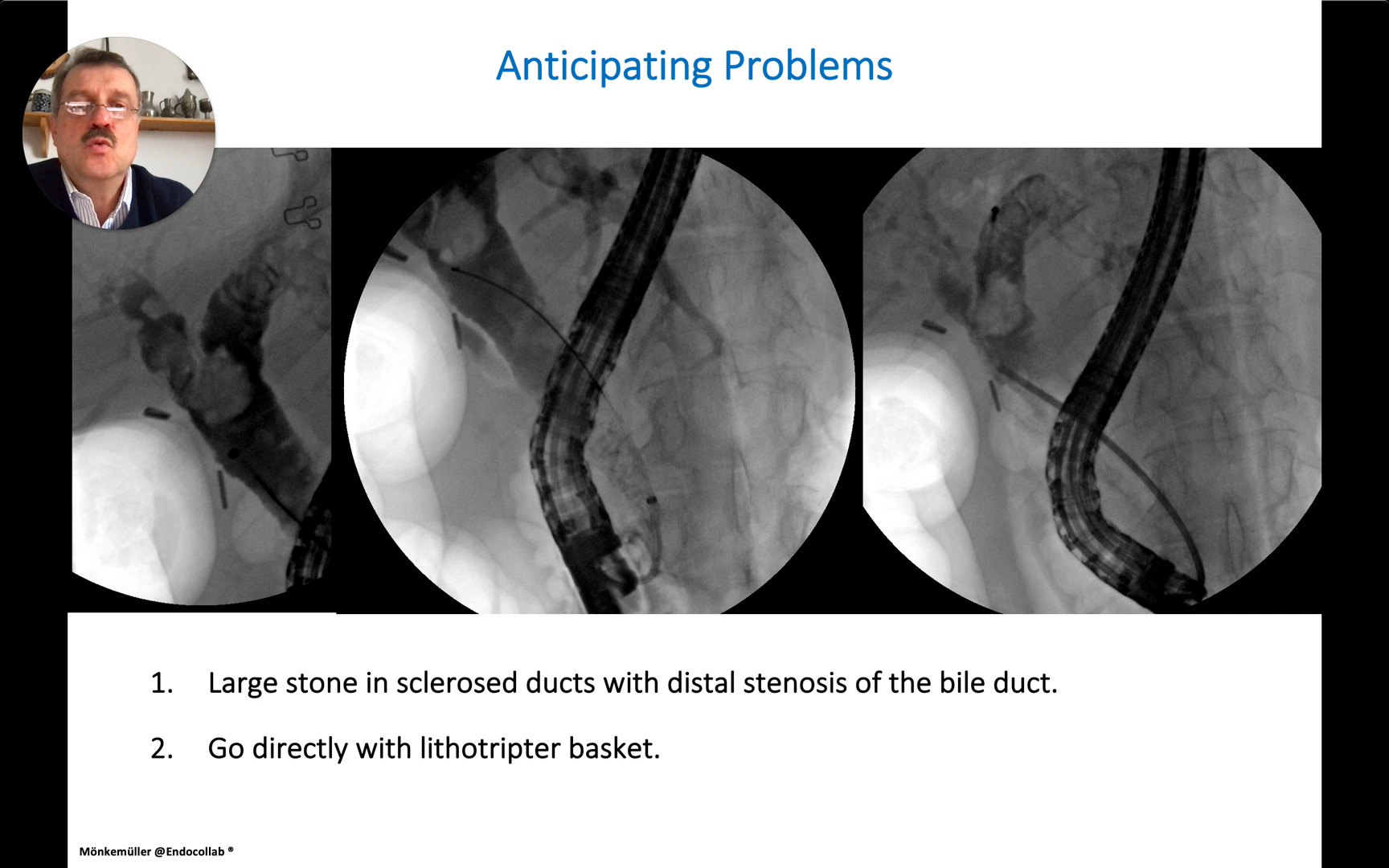
Dr. Mönkemüller instructs endoscopists to evaluate the following parameters on every cholangiogram prior to instrument deployment: the shape and degree of sclerosis of the bile ducts, whether problems are intrahepatic, extrahepatic, or bilateral, the degree of ductal dilation, the presence of any distal stenosis, and the size, shape, number, and consistency of the stones.
The key clinical inference: If a stone appears large, dense, and dark on fluoroscopy—with no yellow gravel emerging—a hard stone should be anticipated.
In that scenario, the speaker recommends proceeding directly with a large sphincterotomy or sphincteroplasty and a lithotripter basket from the outset, rather than attempting standard retrieval first and losing time.
Clinical Pearl: “If you have a stone that is large and looks dark and there is no yellow gravel coming out and you are anticipating a very hard stone, then it’s better to already know that you need to have a big sphincterotomy or sphincteroplasty and go with the lithotripter basket and crush that stone from the beginning. Otherwise, you will be stuck during the procedure for hours and hours.”
Understanding Mechanical Lithotripters: Three Types You Must Know
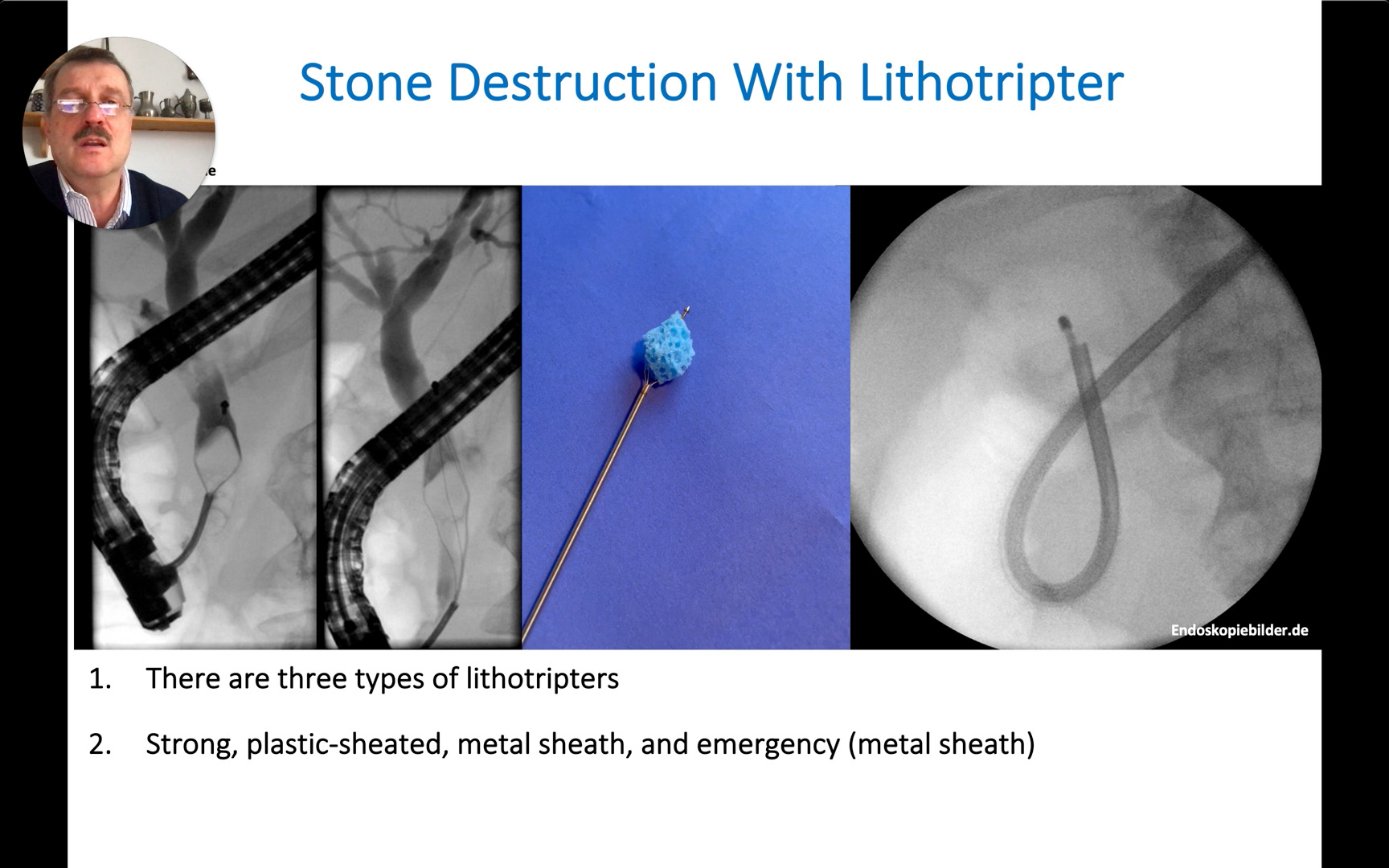
Dr. Mönkemüller identifies three categories of mechanical lithotripter, each suited to a different clinical scenario.
The three lithotripter types:
Strong plastic-sheathed lithotripter — Standard device for planned, through-the-scope lithotripsy.
Metal-sheathed lithotripter — A more robust option for larger stones or tighter ducts.
Emergency (Soehendra) lithotripter — Used when a basket becomes impacted and the endoscope must be removed; does not pass through the scope.
The security tip: Dr. Mönkemüller highlights a critical safety design feature: the distal pin holding the basket wires should be engineered to break off if crushing forces exceed a safe threshold. If the stone cannot be destroyed and this pin does not release, the basket and stone remain permanently impacted—and the patient will require surgical intervention. Selecting a device with this safety mechanism is therefore a patient safety consideration, not merely a technical preference.
Basket Impaction: Who Is at Risk and the Cardinal Rule
Conditions predisposing to basket impaction
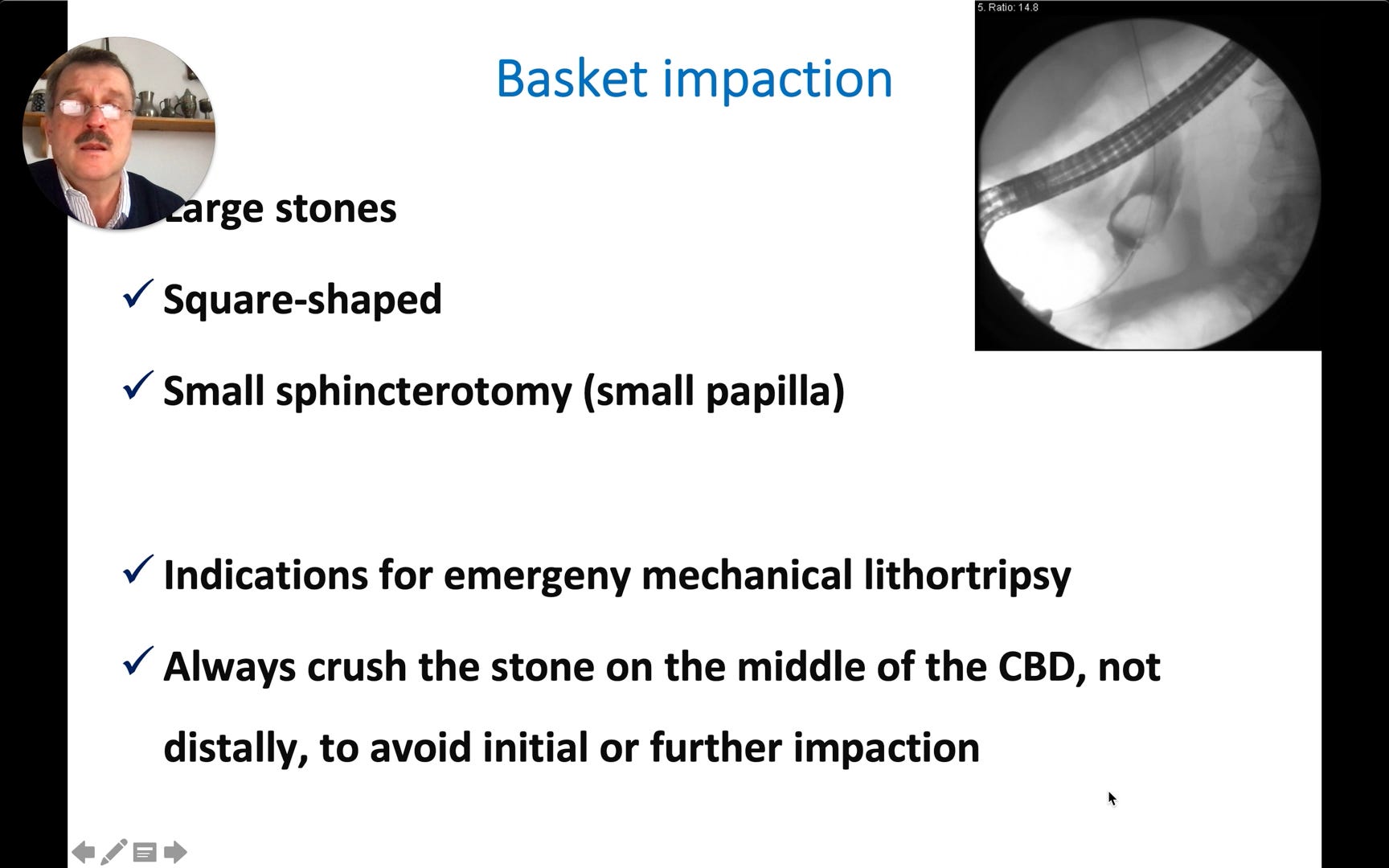
Large stones
Square-shaped stones
Small sphincterotomy (small papilla)
Inadequate sphincterotomy that cannot be enlarged
The speaker reinforces a cardinal technical rule: always attempt to crush the stone in the middle of the CBD (common bile duct), never distally. The distal duct is narrower and is the most likely location for the basket-stone complex to become trapped. Moving the stone proximally before crushing it is a prophylactic maneuver.
⚠️ Warning: “Always crush the stone on the middle of the CBD, not distally, to avoid initial or further impaction.”
To see advanced troubleshooting tips, case variations, and a downloadable quick-reference guide based on this video, consider becoming a paid subscriber.
