

You're performing a colonoscopy when suddenly you realize the bleeding source isn't in the colon—it's somewhere in those 20 feet of small bowel that used to be impossible to reach. Until recently, the small bowel was considered a "black box" [0:06], but device-assisted enteroscopy has changed everything. Whether you choose single balloon, double balloon, or the newer motorized spiral technique can mean the difference between a 30-minute procedure and a 2-hour marathon.
The Evolution from Black Box to Total Access
"Until now, the small bowel has been considered a black box, but since the advent of balloon enteroscopy and then spiral enteroscopy, performing deep enteroscopy became possible" [0:06]. The speaker demonstrates reaching the terminal ileum and entering proximally through the ileocecal valve, then advancing into the cecum—achieving what we now call total enteroscopy [0:20].
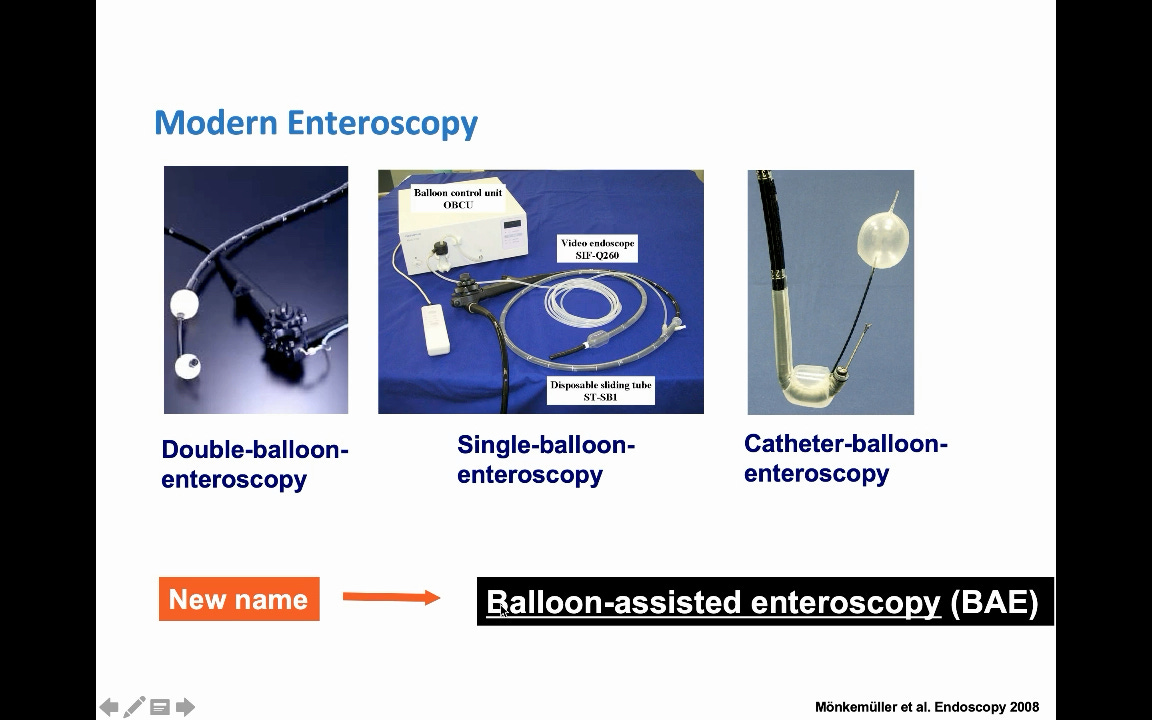
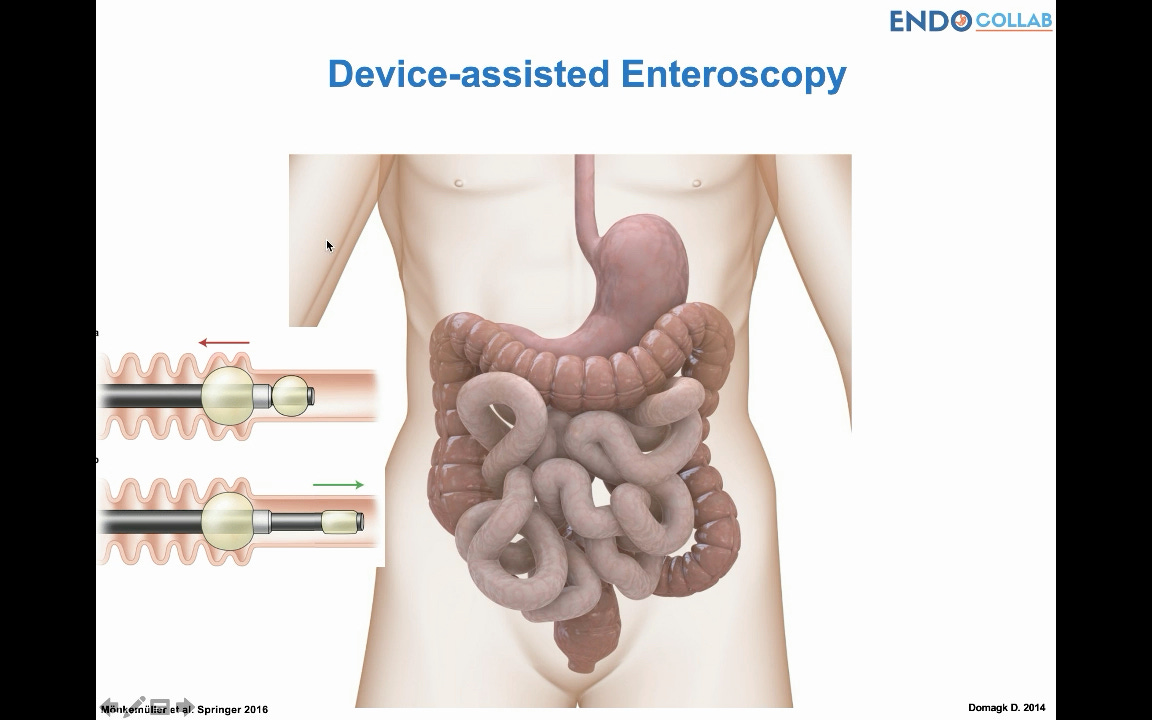
Back in 2008, the terminology evolved from "balloon-assisted enteroscopy" to "device-assisted enteroscopy" to encompass spiral techniques [0:45]. The fundamental principle remains unchanged: keep the examined bowel proximal to the device while leaving the distal portion free for investigation.
The Accordion Principle: Why These Devices Actually Work
Clinical Pearl
"The bowel that has been investigated needs to be kept proximal to the device. This is the key element to remember"
The accordion maneuver—whether using balloons or spiral—stabilizes the proximal bowel while allowing distal advancement [1:30]. This principle underlies all deep enteroscopy techniques.
Double Balloon Technique: The Original Game-Changer
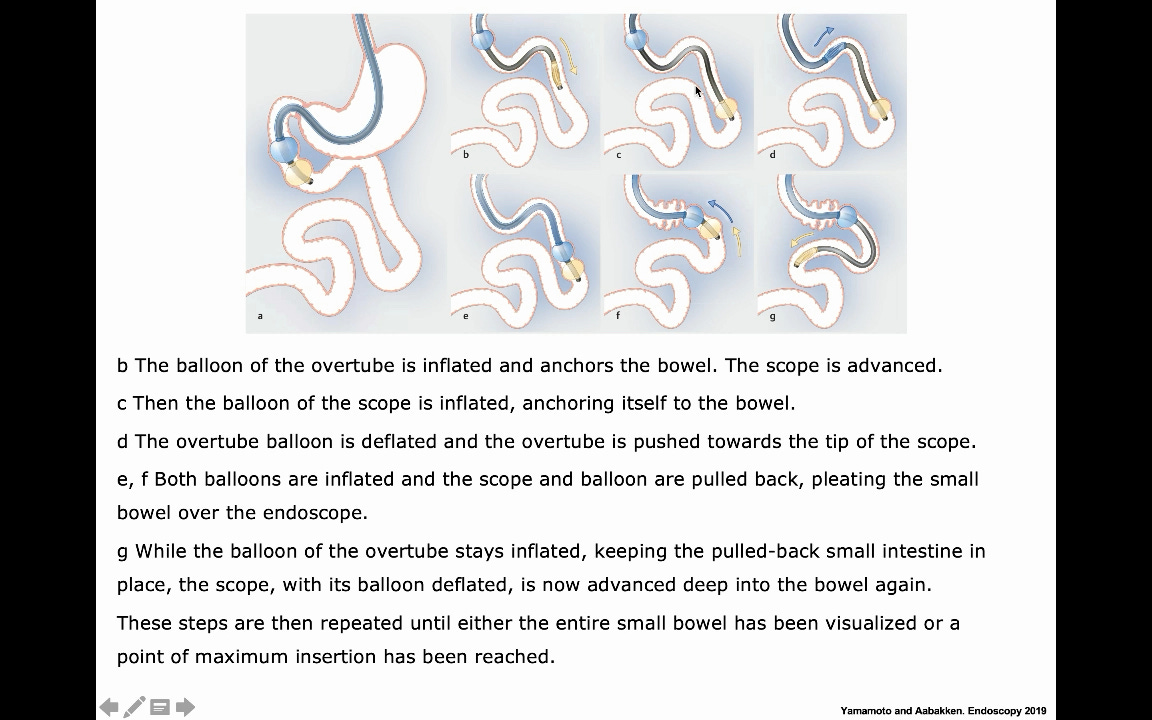
The essential steps for double balloon enteroscopy follow a precise sequence:
Initial stabilization: Inflate both the overtube balloon and scope balloon in the small bowel
Advance the scope: Deflate the endoscope balloon and push forward (the inflated overtube balloon maintains position) [2:00]
Maximum insertion: Reach your limit—"many times can be 40 centimeters, but it is not always that" [2:15]
Overtube advancement: Inflate the scope balloon, deflate the overtube balloon, advance the overtube to meet the scope tip [2:25]
The accordion pull: With overtube balloon inflated, pull both devices back together, pleating the bowel [2:35]
Repeat cycle: Continue stepwise until diagnosis, treatment, or complete enteroscopy is achieved
The speaker notes that full enteroscopy success rates are approximately 5-8% of cases [2:50].
Single Balloon: The Simplified Alternative
The single balloon technique follows the same principle with one crucial difference: "when you have advanced the endoscope, you need to hook it or twist it so that it sort of attaches itself to the bowel wall because there is no balloon here to stabilize it" [3:25].
Pro Tip
Without a balloon on the scope tip, the hooking maneuver becomes critical for maintaining position during overtube advancement [3:30].
Spiral Enteroscopy: Twisting Into the Future
"Spiral enteroscopy actually was a great advancement. As you can see here, you don't need to be pushing and pulling all the time because the procedure is done by twisting the spiral enteroscope which advances into the bowel" [3:50].
The concept appears straightforward, but the speaker cautions: "This sounds easy but it's not always as easy as it is seen in patients who don't have adhesions or problems with bowel obstructions or tumours" [4:05].
