Hi, today we'll learn about upper GI resection techniques for the stomach. This lecture is part of a series on resection techniques for the GI tract and contains many pearls that I'm sure you will enjoy.
The Foundation: Curative vs Diagnostic Resection
Whenever we're doing an endoscopic resection in the stomach, the intent is to do a curative resection. However, here's the first pearl: When performing a diagnostic resection, it does not need to be R0.
There are many conditions where we need to do endoscopic mucosal resection, including:
Polyposis syndromes
Suspected Cronkhite-Canada syndrome
Menetrier's disease
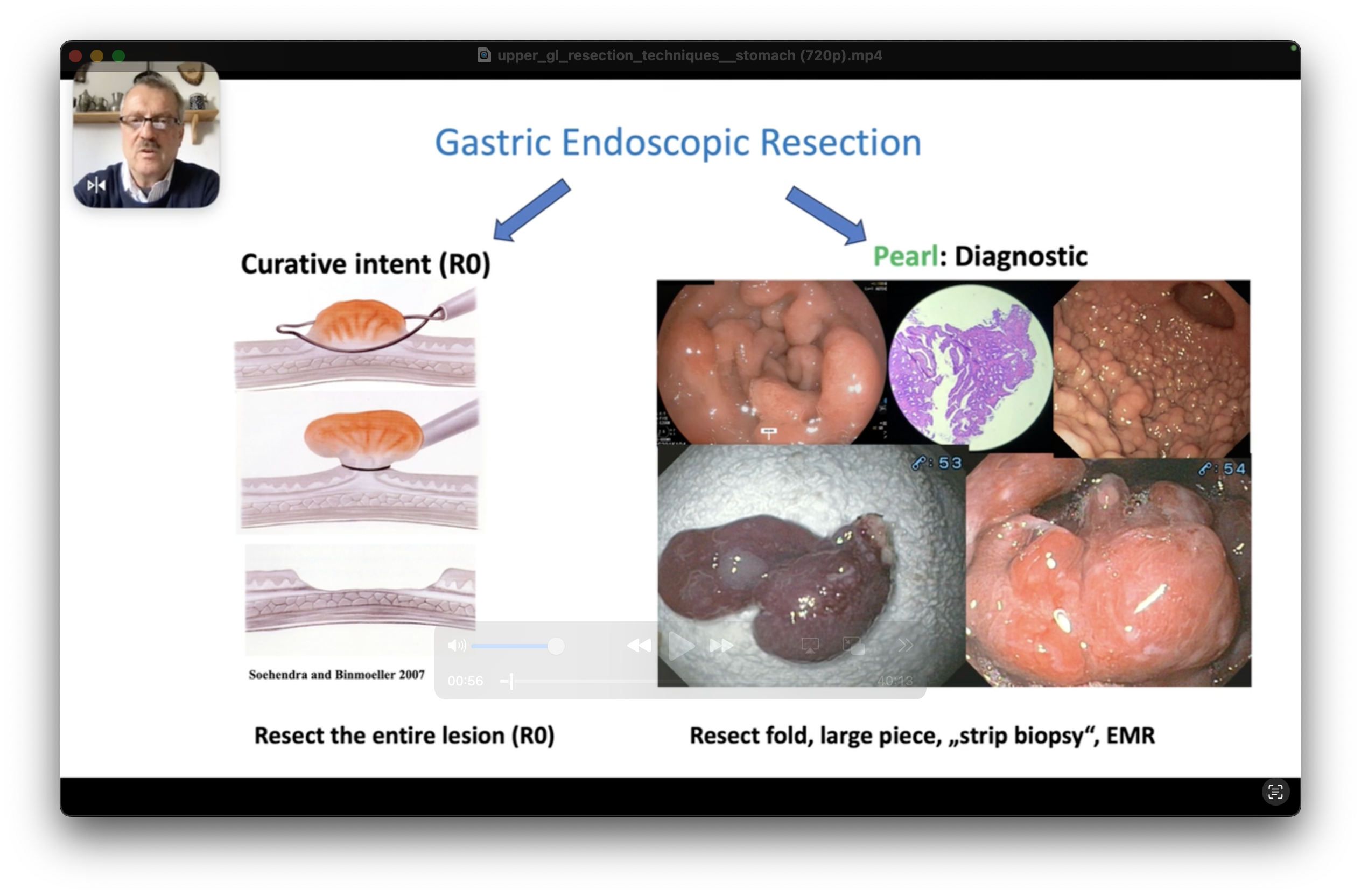
Critical Pearl: Giant Gastric Folds
When you find giant gastric folds, it is much better to do an endoscopic resection of the suspected fold or folds rather than biopsies. Why? Biopsies are really tiny samples of tissues and often the diagnosis will be missed.
Remember: In the fundus, there are no gastric folds—either many or isolated. Therefore, if you see folds in the fundus, it's important that you proceed to do a diagnostic biopsy, in this case, endoscopic mucosal resection. Be careful not to confuse folds with varices—endoscopic ultrasound is often indicated.
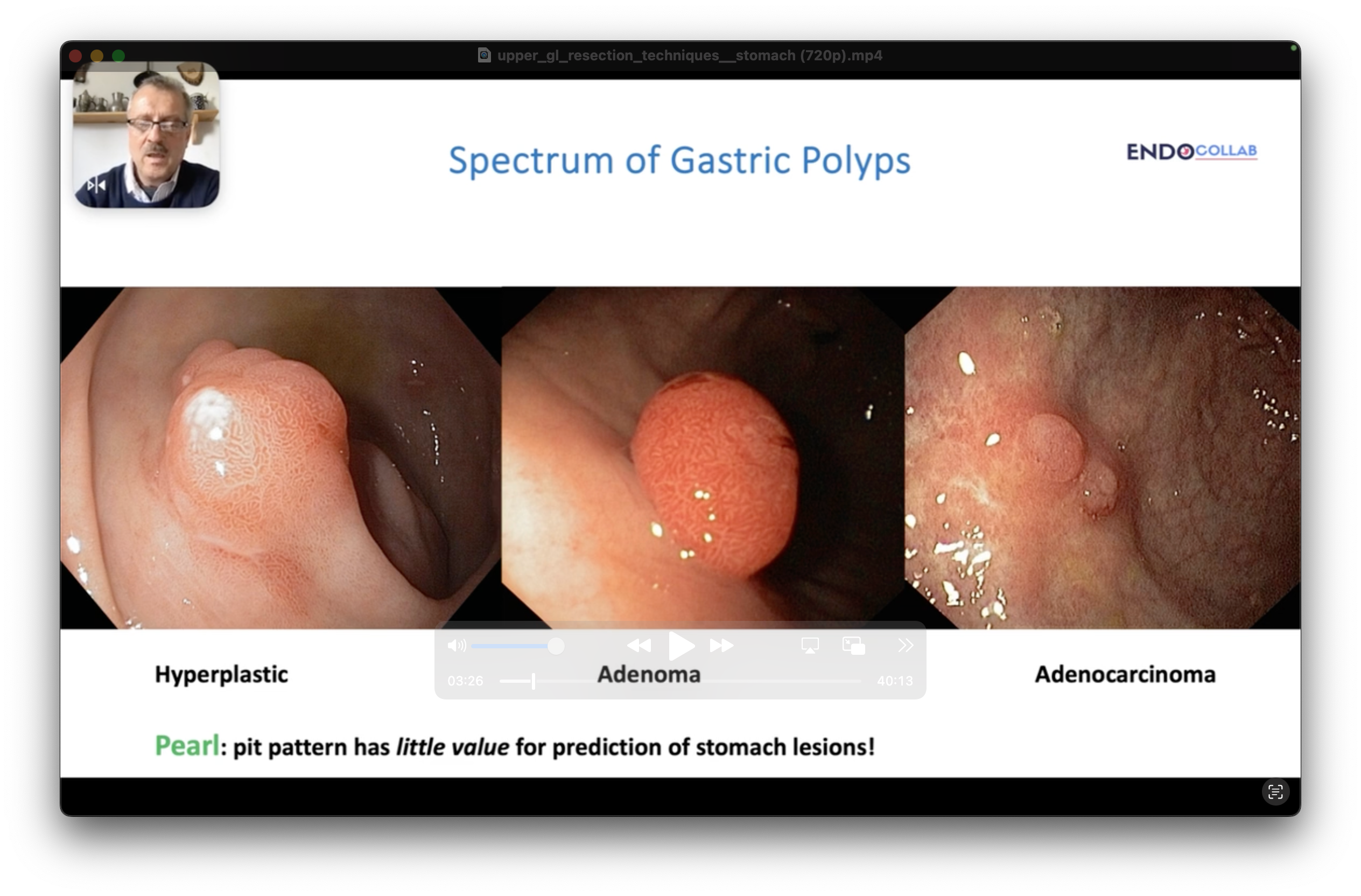
Understanding Gastric Pit Patterns
The pit pattern in the stomach is not the same as the pit pattern prediction of the colon. The mucosa of the stomach is different, the anatomy is different, the presence of acid makes it very difficult to tell based on the pit pattern whether it's hyperplastic or an adenoma or even adenocarcinoma.
Instead, rely better on:
Form of the lesion
Scar presence
Erythema
Presence of multiple lesions